![]()
When Connie Kerrigan became Director of Community Outreach at Parkview Behavioral Health about three and a half years ago—in the midst of the national opioid epidemic—one of her first concerns was that her staff would be emotionally exhausted by the scale of the problem.
“It’s very hard work,” she says. “It’s very hard to keep going in and think: ‘I do something, and then people come back in, and it’s happened again.'”
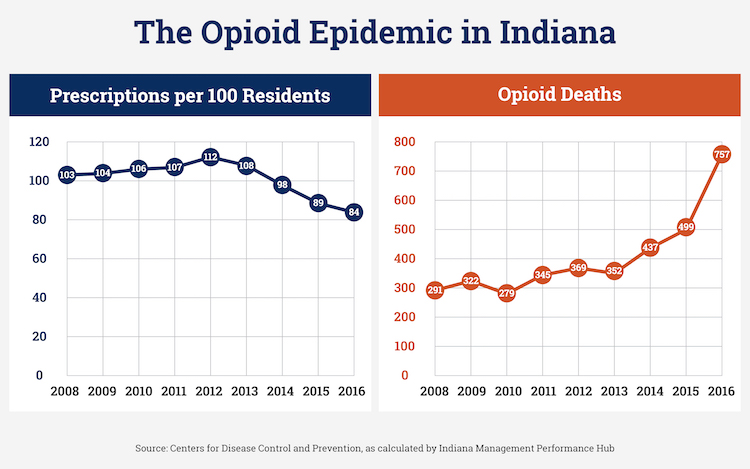
The opioid epidemic is the worst drug crisis in American history and the largest public health crisis. Every day, it kills more than 115 people in the country, and its effects in Allen County are no less frightening.
In 2017, an average of one person died from a drug overdose every three days—with fatal drug poisonings up 70 percent from 2016 alone.

![]() In 2016, there were an average of 115 opioid overdose deaths each day.
In 2016, there were an average of 115 opioid overdose deaths each day.
While street drugs have been an issue in the U.S. for the past 50 years, opioid abuse has been escalating to a national crisis since the late 1990s after a prescription painkiller called OxyContin was introduced to the market in 1996.
It was said to relieve pain for 12-hours, and as such, it became America’s bestselling painkiller, reaping $31 billion in revenue for a drug company called Purdue Pharma (no relation to Purdue University).
But as doctors began prescribing more of it, physicians and consumers alike started noticing a frightening side effect of the drug: It was highly addictive for certain people.
When these people were prescribed opioids, or got their hands on them from someone else, they began to crave them until their cravings consumed their lives, driving them to peddle drugs to afford their addiction, or turn to other drugs, like heroin or fentanyl, to stave off cravings.
“It’s pushed a lot of people to the streets because that’s where it’s cheap and easy to get, and they can manage their withdrawal,” says Shawn Fingerle.
![]()
Like Kerrigan, Fingerle began working for Parkview Behavioral Health about three and a half years ago. In April, he became the center’s first Director of Opioid Treatment and Prevention Services.
His position was created to address the fallout of the opioid epidemic across the Parkview Health Network in northeast Indiana. A large part of his work involves making strategies to help users manage their symptoms as they attempt to recover their lives.
But while people are acutely aware of the effects opioids have and physicians are becoming cautious about prescribing them, prevention is only half of the battle.
Across the country, more than 2.6 million people in the U.S. are already addicted to opioids, and when they try to quit, they experience horrendous withdrawal symptoms known as being “dopesick.”
“Imagine the worst flu you could ever experience,” Fingerle says.

![]() While the opioid epidemic largely started with prescription medication, it is driving users to other drugs like heroin and fentanyl to manage their cravings.
While the opioid epidemic largely started with prescription medication, it is driving users to other drugs like heroin and fentanyl to manage their cravings.
This unprecedented addiction is hollowing out communities across the country, but in northeast Indiana, there are also signs of hope. Parkview Behavioral Health is implementing innovative treatment and recovery plans that promise to reshape regional care for substance abuse.
And it all starts with thinking differently about mental health services, in general.
***
When Kerrigan left nursing and began working at Parkview Behavioral Health, she noticed something strange in region’s mental health services.
She saw a lot of different groups in northeast Indiana working with people to treat “head issues.” But they were all working in silos.
Essentially, people who had “head issues” were being treated differently than people who had “body issues” within the same healthcare system.
“It’s like we cut the head off from the body,” Kerrigan says.
If you had a “body issue,” like heart disease, you could go to your doctor, and they could refer you to specialists, like cardiologists, for treatment.
“It’s all really tied together,” Kerrigan explains. “But if you had a mental health issue, they kind of said, ‘We can send you to Parkview Behavioral Health,’ and that’s it.”
![]()
For years, Parkview Behavioral Health was northeast Indiana’s first line of defense on “head issues” like anxiety, depression, substance addiction, and mood disorders.
But to make Kerrigan’s point, their services for people with addictions were limited. They had alcohol and drug detox programs and an outpatient day program. But they didn’t have residential programs or support groups.
Instead, these programs were housed at other regional care centers like Park Center, creating gaps and silos within the system.
“With addictions, you don’t want there to be gaps,” Fingerle says. “You’ve got to have an airtight plan for people to follow.”
So as the opioid epidemic evolves across the region, northeast Indiana’s mental health services are evolving, too.
On October 1, all of Park Center’s locations will become affiliates of Parkview Health, helping people across the region get a wider range of care faster and closer to home.
“This addiction is happening in all the communities, in all the offices everywhere, so we really need to have a strategy that addresses it where it shows up—not just at Parkview Behavioral Health in Fort Wayne,” Fingerle says.
As Parkview's comprehensive mental health services extend across the region, they're taking the opportunity to implement unified, innovative approaches to the opioid epidemic, as well.
***
Since the height of drug hysteria in the 1980s, the decision to do drugs has largely been portrayed as a moral choice.
The message comes to us in movies and music, afterschool specials and religious programs, peer pressure situations and conversations with well-meaning parents.
Doing drugs is a “bad” decision, and as such, the culture we live in often qualifies drug abusers as “bad people.”
But what if the decision to do drugs—or rather to keep doing them—was less of an indication of someone’s moral compass and more of a chronic condition that affects certain people, like asthma or diabetes?
That’s what substance abuse specialists are starting to discover.
“This is really a brain disorder,” Finglerle says. “People haven’t really looked at it that way. They’ve looked at it more as a choice or a moral failing. But we know that opioids actually alter chemistry in the brain and make it hard for users to quit.”

![]() Substance abuse specialists are starting to treat drug addiction as a brain disorder.
Substance abuse specialists are starting to treat drug addiction as a brain disorder.
That means people's cravings for opioids and other drugs are real, Fingerle says, and traditional abstinence-only recovery models that focus on willpower and moral choices aren’t working for nation’s influx of opioid addicts.
To get better results and keep patients alive longer, healthcare professionals are turning to medical-assisted therapies (MAT) as a way to treat drug addiction instead.
According to the Substance Abuse and Mental Health Services Administration, MAT involves using FDA-approved medications in combination with counseling and behavioral therapies to provide a “whole-patient approach" to substance disorders.
In 2015, one of the first long-term follow-ups of patients treated with MAT for opioid addiction showed that 50 percent were abstinent after 18 months, and beyond that, the success rate continues to grow.
"After 3.5 years, the portion who reported being abstinent had risen further, to 61 percent, and fewer than 10 percent met diagnostic criteria for dependence on the drugs," the National Institute on Drugs reports.
These numbers are particularly encouraging compared to the peer-reviewed success rate of traditional abstinence programs like Alcoholics Anonymous and Narcotics Anonymous, which fall somewhere between five and 10 percent.
But the problem with treating a medication addiction with more medication is that there’s a stigma attached to it.
Critics see MAT as merely another form of addiction, replacing one drug with another, and even they accept it, MAT still doesn't work for about 40 percent of opioid users, so it's not a one-size-fits-all solution or a "magic cure," Fingerle says.
Even so, MAT may be the first important step in helping more than half of the nation's opioid addicts recover their lives because it allows them to calm their brains enough to focus, and understanding the science of that can be simple, Kerrigan explains.
Imagine a wagon traveling down a muddy path. That is a drug user’s brain on drugs, and the more often they do drugs, the deeper those ruts get, she explains, making it harder for them to quit by sheer willpower.
Even with the most effective therapy possible, as long as the wagon is still stuck in the rut, it’s going to be hard for the addicted person to make a lasting change.
“Their brain is just not wired in such a way to really resist it,” she says.

![]() Kerrigan compares an opioid user's brain to a wagon traveling down a muddy path. The more often they do drugs, the deeper the ruts in their mind get, keeping them stuck in the same patterns.
Kerrigan compares an opioid user's brain to a wagon traveling down a muddy path. The more often they do drugs, the deeper the ruts in their mind get, keeping them stuck in the same patterns.
However, if a medication can intervene to help people get out of the rut and set their wheels on a fresh path, then therapies have the ability to be more effective. People can even start rewiring their brains by filling in the ruts their addictions created.
“The addiction is always there,” Kerrigan says. “But with all your strategies and the more success you have, those ruts get less deep, so you’re not as likely to get in that path again.”
As such, Parkview Behavioral Health is recommending MAT as part of its continuum of care.
“What we say is, MAT is important in combination with therapy,” Fingerle explains. “That’s where you have your best possibility of success, and your best outcomes after a year.”
Thanks to positive results with this approach, Fingerle says opinions on MAT are starting to shift across the northeast Indiana region, too.
“We just came out of a meeting where, a year or two ago, they would have been against MAT,” he says. “Now they’re all moving toward being supportive because the data is there. These medications are going to keep people alive longer, and they’re going to have a better chance of staying sober.”
***
Along with MAT, Fingerle believes the realization that drug addiction is a brain disorder has huge implications for drug users and healthcare professionals alike, particularly when it comes to relapses along the road to recovery.
For users, thinking of drug addiction as a brain disorder means relapsing does not make them “failures” or “bad people,” but instead indicates that their disorder is part of a chronic condition.
For healthcare professionals, it means recognizing that there are reasons to have hope despite setbacks in the treatment regimen.
At Parkview Behavioral Health, there are four levels of addiction treatment based on people’s needs, from most acute to least acute.
When someone is first trying to quit, there’s hospitalization for detox and withdrawal management. Then, there’s residential living arrangements that typically last for 30 days to help people stay sober the first month. After that, they might be in partial hospitalization or intensive outpatient care where they’re coming in several times a week for several hours of treatment. Finally, as people recover, they might attend therapies and support groups that help them maintain their abstinence.
But while this four-tiered approach completes the continuum of care, Kerrigan says the path to sobriety is often not linear or timely.
“It could really take several years before they’re stable, and sometimes people will go back and use again and then get back on track,” she says. “Addiction is a chronic disease, so we expect that.”
![]()
She explains that when you’re treating any chronic condition, like asthma or heart disease, some people will have a flare-up in recovery, and others won’t. It’s just how chronic conditions work.
Fingerle hopes that as the public and the healthcare community start to see drug addiction as a brain disorder and a chronic condition, they will think differently about relapses, too.
“We’ve had incidences where people have relapsed two or three times with drug addiction, and people say, ‘We’re done. You just keep relapsing, so we’re done,’” Fingerle says. “But would we ever do that with somebody who’s had three heart attacks?”
Asking critical questions like these will be instrumental in changing the stigma around substance addiction as northeast Indiana moves forward, he explains. And while the road to recovery will be long and winding, healthcare professionals like Kerrigan are starting to see signs of hope.
“Funding is lining up, treatment is lining up—all those pieces are starting to come together,” she says. “I don’t know that we’ve hit our peak yet, but I feel that we are starting to make much better connections.”
This Special Report was made possible by Parkview Health.